ACE Inhibitors
Angiotensin-converting enzyme (ACE) inhibitors are now the established first-line treatment in younger patients with hypertension and are also extensively used to treat heart failure. They are known to be less effective in treating hypertensive Afro-Caribbean patients. ACE inhibitors are also used to treat diabetic nephropathy and have a role in the secondary prevention of ischaemic heart disease.
Mechanism of action:
- inhibit the conversion angiotensin I to angiotensin II
- ACE inhibitors are activated by phase 1 metabolism in the liver
Side-effects:
- cough
- occurs in around 15% of patients and may occur up to a year after starting treatment
- thought to be due to increased bradykinin levels
- angioedema: may occur up to a year after starting treatment
- hyperkalaemia
- first-dose hypotension: more common in patients taking diuretics
Cautions and contraindications
- pregnancy and breastfeeding - avoid
- renovascular disease - may result in renal impairment
- aortic stenosis - may result in hypotension
- hereditary of idiopathic angioedema
- specialist advice should be sought before starting ACE inhibitors in patients with a potassium >= 5.0 mmol/L
Interactions
- patients receiving high-dose diuretic therapy (more than 80 mg of furosemide a day)
- significantly increases the risk of hypotension
Monitoring
- urea and electrolytes should be checked before treatment is initiated and after increasing the dose
- a rise in the creatinine and potassium may be expected after starting ACE inhibitors
- acceptable changes are an increase in serum creatinine, up to 30% from baseline and an increase in potassium up to 5.5 mmol/l.
- significant renal impairment may occur in patients who have undiagnosed bilateral renal artery stenosis
 | |
| |
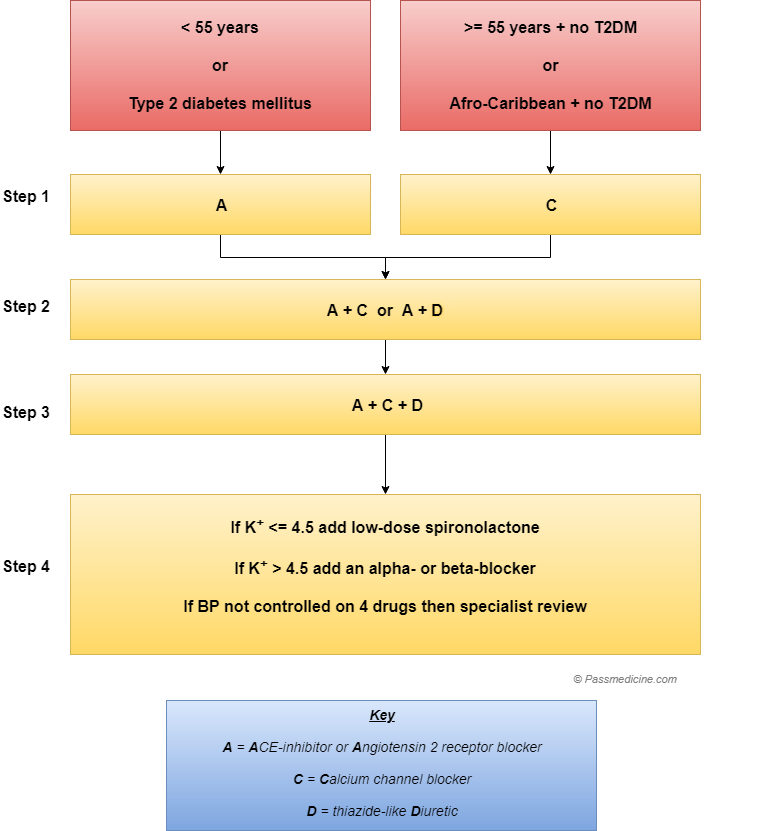
Flow chart showing the management of hypertension as per current NICE guideliness