Parkinsons Management
Parkinson's disease: management
Parkinsons disease should only be diagnosed, and management initiated, by a specialist with expertise in movement disorders. However, it is important for all doctors to be aware of the medications used in Parkinson's given the prevalence of this condition. NICE published guidelines in 2017 regarding the management of Parkinson's disease.
For first-line treatment:
- if the motor symptoms are affecting the patient's quality of life: levodopa
- if the motor symptoms are not affecting the patient's quality of life: dopamine agonist (non-ergot derived), levodopa or monoamine oxidase B (MAO‑B) inhibitor
Whilst all drugs used to treat Parkinson's can cause a wide variety of side-effects NICE produced tables to help with decision making:
| Levodopa | Dopamine agonists | MAO‑B inhibitors | |
|---|---|---|---|
| Motor symptoms | More improvement in motor symptoms | Less improvement in motor symptoms | Less improvement in motor symptoms |
| Activities of daily living | More improvement in activities of daily living | Less improvement in activities of daily living | Less improvement in activities of daily living |
| Motor complications | More motor complications | Fewer motor complications | Fewer motor complications |
| Adverse events | Fewer specified adverse events* | More specified adverse events* | Fewer specified adverse events* |
| * excessive sleepiness, hallucinations and impulse control disorders |
If a patient continues to have symptoms despite optimal levodopa treatment or has developed dyskinesia then NICE recommend the addition of a dopamine agonist, MAO‑B inhibitor or catechol‑O‑methyl transferase (COMT) inhibitor as an adjunct. Again, NICE summarise the main points in terms of decision making:
| Dopamine agonists | MAO‑B inhibitors | COMT inhibitors | Amantadine | |
|---|---|---|---|---|
| Motor symptoms | Improvement in motor symptoms | Improvement in motor symptoms | Improvement in motor symptoms | No evidence of improvement in motor symptoms |
| Activities of daily living | Improvement in activities of daily living | Improvement in activities of daily living | Improvement in activities of daily living | No evidence of improvement in activities of daily living |
| Off time | More off‑time reduction | Off‑time reduction | Off‑time reduction | No studies reporting this outcome |
| Adverse events | Intermediate risk of adverse events | Fewer adverse events | More adverse events | No studies reporting this outcome |
| Hallucinations | More risk of hallucinations | Lower risk of hallucinations | Lower risk of hallucinations | No studies reporting this outcome |
Specific points regarding Parkinson's medication
NICE reminds us of the risk of acute akinesia or neuroleptic malignant syndrome if medication is not taken/absorbed (for example due to gastroenteritis) and advise against giving patients a 'drug holiday' for the same reason.
Impulse control disorders have become a significant issue in recent years. These can occur with any dopaminergic therapy but are more common with:
- dopamine agonist therapy
- a history of previous impulsive behaviours
- a history of alcohol consumption and/or smoking
If excessive daytime sleepiness develops then patients should not drive. Medication should be adjusted to control symptoms. Modafinil can be considered if alternative strategies fail.
If orthostatic hypotension develops then a medication review looking at potential causes should be done. If symptoms persist then midodrine (acts on peripheral alpha-adrenergic receptors to increase arterial resistance) can be considered.
Consider glycopyrronium bromide to manage drooling of saliva in people with Parkinson's disease.
Further information regarding specific anti-Parkinson's medication
Levodopa
- nearly always combined with a decarboxylase inhibitor (e.g. carbidopa or benserazide)
- this prevents the peripheral metabolism of levodopa to dopamine outside of the brain and hence can reduce side effects
- common adverse effects:
- dry mouth
- anorexia
- palpitations
- postural hypotension
- psychosis
- some adverse effects are due to the difficulty in achieving a steady dose of levodopa
- end-of-dose wearing off: symptoms often worsen towards the end of dosage interval. This results in a decline of motor activity
- 'on-off' phenomenon: large variations in motor performance, with normal function during the ‘on’ period, and weakness and restricted mobility during the ‘off’ period
- dyskinesias at peak dose: dystonia, chorea and athetosis (involuntary writhing movements)
- these effects may worsen over time with - clinicians therefore may limit doses until necessary
- it is important not to acutely stop levodopa, for example, if a patient is admitted to hospital
- if a patient with Parkinson's disease cannot take levodopa orally, they can be given a dopamine agonist patch as rescue medication to prevent acute dystonia
Dopamine receptor agonists
- e.g. bromocriptine, ropinirole, cabergoline, apomorphine
- ergot-derived dopamine receptor agonists (bromocriptine, cabergoline) have been associated with pulmonary, retroperitoneal and cardiac fibrosis. The Committee on Safety of Medicines advice that an echocardiogram, ESR, creatinine and chest x-ray should be obtained prior to treatment and patients should be closely monitored
- patients should be warned about the potential for dopamine receptor agonists to cause impulse control disorders and excessive daytime somnolence
- more likely than levodopa to cause hallucinations in older patients. Nasal congestion and postural hypotension are also seen in some patients
MAO-B (Monoamine Oxidase-B) inhibitors
- e.g. selegiline
- inhibits the breakdown of dopamine secreted by the dopaminergic neurons
Amantadine
- mechanism is not fully understood, probably increases dopamine release and inhibits its uptake at dopaminergic synapses
- side-effects include ataxia, slurred speech, confusion, dizziness and livedo reticularis
COMT (Catechol-O-Methyl Transferase) inhibitors
- e.g. entacapone, tolcapone
- COMT is an enzyme involved in the breakdown of dopamine, and hence may be used as an adjunct to levodopa therapy
- used in conjunction with levodopa in patients with established PD
Antimuscarinics
- block cholinergic receptors
- now used more to treat drug-induced parkinsonism rather than idiopathic Parkinson's disease
- help tremor and rigidity
-
e.g. procyclidine, benzotropine, trihexyphenidyl (benzhexol)
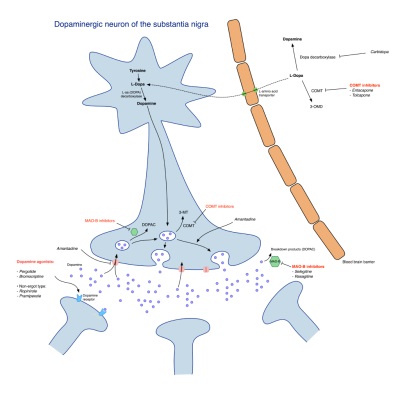
Image sourced from Wikipedia 

Diagram showing the mechanism of action of Parkinson's drugs